![]()
[2026] CPHQ Answers CPHQ Free Demo Are Based On The Real Exam
CPHQ [Mar-2026 Newly Released] Exam Questions For You To Pass
NEW QUESTION # 166
The data below shows 30-day readmission rates for heart failure patients by the primary language spoken and by gender with 95% confidence intervals in parentheses. Which group should be the priority target for reducing disparities in readmission rates?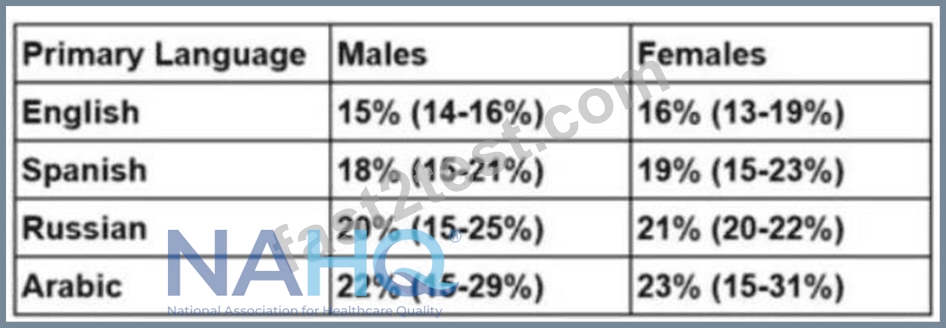
- A. All Russian speakers
- B. Russian-speaking females
- C. All Arabic speakers
- D. Arabic-speaking females
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract:
The goal is to identify the group with the greatest disparity in 30-day readmission rates for heart failure patients, focusing on primary language and gender, to prioritize interventions for reducing disparities. NAHQ CPHQ study materials emphasize that addressing disparities in population health involves targeting groups with the highest rates of adverse outcomes, such as readmissions, to achieve health equity. Disparities are often influenced by social determinants of health, including language barriers, which can affect communication, understanding of discharge instructions, and access to follow-up care.
The data shows readmission rates by language and gender, with 95% confidence intervals indicating the range of uncertainty around the point estimates. Let's analyze the rates:
* English: Males 15% (14-16%), Females 16% (13-19%)
* Spanish: Males 18% (15-21%), Females 19% (15-23%)
* Russian: Males 20% (15-25%), Females 21% (20-22%)
* Arabic: Males 22% (15-29%), Females 23% (15-31%)
First, compare the point estimates across groups. Arabic-speaking patients have the highest readmission rates:
22% for males and 23% for females, followed by Russian-speaking patients at 20% for males and 21% for females. English-speaking patients have the lowest rates at 15% for males and 16% for females. The confidence intervals show overlap between groups (e.g., Arabic males 15-29% overlaps with Russian males
15-25%), but the point estimates provide a clear ranking, with Arabic speakers consistently highest.
To assess disparities, calculate the overall rates for language groups by averaging male and female rates (since the options include "All Arabic speakers" and "All Russian speakers"):
* Arabic speakers: (22% + 23%) / 2 = 22.5%
* Russian speakers: (20% + 21%) / 2 = 20.5%
* Spanish speakers: (18% + 19%) / 2 = 18.5%
* English speakers: (15% + 16%) / 2 = 15.5%
Arabic speakers have the highest average readmission rate (22.5%), indicating the greatest disparity compared to English speakers (15.5%), a difference of 7 percentage points. Russian speakers have a 20.5% average rate, a 5-point difference from English speakers.
Now, compare the gender-specific options: Arabic-speaking females (A) have a rate of 23%, and Russian- speaking females (B) have a rate of 21%. While Arabic-speaking females have the highest single rate, the question asks for the priority group to reduce disparities, which often involves targeting the broadest group with the largest overall disparity. Option C, "All Arabic speakers," encompasses both males (22%) and females (23%), with an average of 22.5%, making it the group with the most significant disparity across both genders. Option D, "All Russian speakers," has a lower average rate (20.5%).
The confidence intervals, while wide for smaller groups like Arabic and Russian speakers, do not change the prioritization, as the point estimates consistently show Arabic speakers with the highest rates. NAHQ emphasizes targeting the group with the greatest disparity in outcomes to address health equity, particularly when language barriers (e.g., Arabic speakers) may contribute to higher readmissions due to communication challenges. Therefore, "All Arabic speakers" (C) should be the priority target for interventions, such as language-specific education or interpreter services, to reduce disparities in readmission rates.
Reference: NAHQ CPHQ Study Guide, Population Health and Care Transitions Section, "Addressing Health Disparities in Readmissions"; NAHQ CPHQ Practice Exam, Population Health Data Analysis for Equity.
NEW QUESTION # 167
A department analyzed Its process for distributing paychecks to employees. The analysis showed there were multiple checkpoints tor approval, delays In processing of the checks, and errors that caused extra work for staff. Which of the following types of waste were identified during the analysis?
- A. defects, waiting, and over processing
- B. waiting. Inventory, and transportation
- C. Inventory, variation, and motion
- D. variation, overproduction, and over processing
Answer: A
Explanation:
The question is about identifying types of waste in a process. In the context of Lean methodology, which is often applied in healthcare quality improvement, waste is any activity that doesn't add value to the end product or service1.
In the given scenario, the process for distributing paychecks to employees was analyzed and the following issues were identified:
* Multiple checkpoints for approval
* Delays in processing of the checks
* Errors that caused extra work for staff
These issues can be mapped to the following types of waste:
* Defects: Errors that cause extra work fall under this category. In this case, the errors in the paycheck distribution process that resulted in additional work for the staff are considered defects1.
* Waiting: Delays in processing checks represent the waste of waiting. This refers to the time wasted waiting for the next step in a process1.
* Overprocessing: Having multiple checkpoints for approval can be seen as overprocessing, which refers to doing more work than needed1.
Therefore, the types of waste identified during the analysis are defects, waiting, and overprocessing, which corresponds to option B. This answer is verified as per healthcare quality documents and learning resources1.
NEW QUESTION # 168
Which of the following best describes the technique of assessing the current level of performance and comparing it to the desired level of performance?
- A. Gap analysis
- B. SIPOC
- C. Work breakdown structure
- D. Qualitative analysis
Answer: A
Explanation:
The NAHQ CPHQ competency framework defines gap analysis as a structured method for comparing an organization's current state with a desired future state. It identifies performance gaps and informs prioritization of improvement activities.
Option C is correct because gap analysis directly evaluates discrepancies between actual and target performance, which is foundational in quality planning and accreditation readiness.
SIPOC maps processes at a high level. Work breakdown structures decompose project tasks. Qualitative analysis interprets non-numeric data.
The CPHQ exam emphasizes gap analysis as an essential tool for strategic planning, performance improvement, and compliance efforts.
NEW QUESTION # 169
Which of the following interventions has the greatest potential for positive impact due to its ability to address social determinants of health?
- A. worksite obesity prevention program
- B. tobacco control interventions
- C. access to clean syringes
- D. public transportation system expansion
Answer: D
Explanation:
Public transportation system expansion (A) addresses a key social determinant of health (transportation barriers), improving access to healthcare, employment, and healthy food, with broad population impact. Clean syringes (B), tobacco control (C), and obesity programs (D) have narrower scopes. NAHQ prioritizes systemic SDOH interventions.
NAHQ CPHQ Study Guide, Population Health and Care Transitions Section, "Social Determinants of Health Interventions"; NAHQ CPHQ Practice Exam, Population Health Strategies.
NEW QUESTION # 170
Which of the following is an example of using human factors engineering to improve patient safety?
- A. performing a root cause analysis on events of harm
- B. using checklists to complete complicated tasks
- C. providing simulation training for high-risk patient care tasks
- D. having a second person check medication calculations
Answer: B
Explanation:
Human factors engineering focuses on designing systems and processes that account for human capabilities and limitations to improve safety and performance. Using checklists to complete complicated tasks (Answer D) is a prime example of applying human factors engineering to enhance patient safety.
Checklists help ensure that critical steps in a process are not overlooked, reducing the likelihood of errors, especially in high-risk, complex tasks such as surgical procedures or medication administration.
The other options, while important for patient safety, do not specifically represent human factors engineering:
Performing a root cause analysis on events of harm (A) is an investigative process for identifying underlying causes of errors, not a human factors engineering intervention.
Providing simulation training for high-risk patient care tasks (B) is an educational approach to improving skills and preparedness, not directly related to system design.
Having a second person check medication calculations (C) is a safety double-check but is more of a verification process than a systemic design change.
Reference: National Association for Healthcare Quality (NAHQ) - Certified Professional in Healthcare Quality (CPHQ) Study Materials.
Human Factors Engineering in Healthcare, NAHQ Documentation.
NEW QUESTION # 171
The quality professional has been tasked to conduct focus groups to gather more information on culture of safety. What kind of data will this yield?
- A. Quantitative
- B. Continuous
- C. Qualitative
- D. Discrete
Answer: C
Explanation:
Focus groups collect subjective insights, opinions, and experiences, typically used to assess perceptions like safety culture.
Option A (Continuous): Continuous data involves measurable quantities (e.g., time), not focus group opinions.
Option B (Quantitative): Quantitative data is numerical (e.g., survey scores), not the narrative data from focus groups.
Option C (Discrete): Discrete data involves countable categories, not open-ended focus group responses.
Option D (Qualitative): This is the correct answer. The NAHQ CPHQ study guide states, "Focus groups yield qualitative data, capturing subjective insights and perceptions, such as staff views on safety culture" (Domain
2).
CPHQ Objective Reference: Domain 2: Health Data Analytics, Objective 2.1, "Classify data types," includes qualitative data from focus groups. The NAHQ study guide notes, "Qualitative data is key for assessing safety culture" (Domain 2).
Rationale: Focus groups provide qualitative data, aligning with CPHQ's analytics principles.
Reference: NAHQ CPHQ Study Guide, Domain 2: Health Data Analytics, Objective 2.1.
NEW QUESTION # 172
Because of the goals of care can be defined broadly, outcome measures have come to include the costs of care as well as patients' satisfaction with care.
In formulations that stress the technical aspects of care, however outcome typically refers to:
- A. Special set of clinical activities
- B. Health status-related indicators such as whether the pain subsided
- C. Appropriate and potentially harmless care
- D. Desired results
Answer: B
NEW QUESTION # 173
A treatment center has experienced an increasing number of adverse medication safety events. Review of the data shows a medication error rate for drug-drug interactions of 15.7 per 1,000 medications dispensed. The organizational goal is less than 5 per 1,000, and ultimately 0. Which of the following solutions is most appropriate to consider?
- A. Human factors engineering
- B. Computerized order entry
- C. Barcode medication administration
- D. Electronic medical record implementation
Answer: B
Explanation:
The NAHQ CPHQ exam blueprint emphasizes matching patient safety interventions to the specific failure mode. Drug-drug interaction errors most commonly occur at the ordering stage, making computerized provider order entry (CPOE) with clinical decision support the most effective intervention.
Option A is correct because CPOE systems provide real-time alerts for drug-drug interactions, allergies, and contraindications at the point of prescribing, preventing errors before medications are dispensed or administered.
Human factors engineering (Option B) supports system design but is not a discrete solution for interaction checking. Electronic medical records alone (Option C) do not necessarily include active interaction alerts.
Barcode medication administration (Option D) occurs at the administration phase and does not address prescribing-related interaction errors.
The CPHQ framework prioritizes upstream, system-level controls that prevent harm rather than detecting it later, making CPOE the most appropriate solution.
NEW QUESTION # 174
During a regulatory survey, an organization received deficiencies in the handling of medical waste. What is the organization's next step?
- A. Develop a targeted action plan on medical waste handling.
- B. Update the policy on medical waste handling.
- C. Educate frontline staff on handling medical waste.
- D. Validate compliance with the updated medical waste handling process.
Answer: A
Explanation:
Explanation: Developing a targeted action plan (D) is the next step to address medical waste handling deficiencies, outlining interventions and timelines. Education (A), policy updates (C), and compliance validation (B) follow planning. NAHQ emphasizes action planning for survey deficiencies.
NAHQ CPHQ Study Guide, Performance and Process Improvement Section, "Responding to Regulatory Survey Deficiencies"; NAHQ CPHQ Practice Questions, Compliance and Corrective Actions.
NEW QUESTION # 175
A multidisciplinary team has been convened to review delays in laboratory turnaround time between the medicine clinic and the laboratory. The team's first step in evaluating the issue is to
- A. observe how the medical assistants prepare the specimens.
- B. see if the surgery clinic is also experiencing delays.
- C. conduct a failure mode and effects analysis (FMEA).
- D. create a flow chart to study the process.
Answer: D
Explanation:
The first step for a multidisciplinary team tasked with evaluating delays in laboratory turnaround time is to create a flow chart to study the process. A flow chart visually maps out the steps involved in the current process, allowing the team to understand each stage, identify bottlenecks, and pinpoint where delays might be occurring. This provides a clear, shared understanding of the process among all team members, which is essential before diving into more detailed analysis or improvements.
* Conduct a failure mode and effects analysis (FMEA) (B): FMEA is a valuable tool for identifying potential failures, but it is typically used after understanding the process in detail.
* See if the surgery clinic is also experiencing delays (C): While this could be useful information, the primary focus should be on the specific process under review.
* Observe how the medical assistants prepare the specimens (D): Observation is important, but understanding the entire process flow is the first step.
References
* NAHQ Body of Knowledge: Process Mapping and Flowcharting in Quality Improvement
* NAHQ CPHQ Exam Preparation Materials: Initial Steps in Process Improvement
=========
NEW QUESTION # 176
A root cause analysts (RCA) was conducted tor an event related to a delayed high-priority alarm response.
Alarm fatigue was determined to be a root cause. Which of the following Is the most appropriate first Intervention?
- A. Review alarm signals for clinical appropriateness.
- B. Establish a written policy for alarms escalation.
- C. Implement a guideline with clear criteria for Initiation of cardiac monitoring.
Answer: A
Explanation:
* A root cause analysis (RCA) is a systematic process of identifying the factors that contributed to an adverse event or near miss in order to prevent recurrence and improve patient safety1.
* Alarm fatigue is a condition in which clinicians become desensitized to the numerous alerts and warnings generated by medical devices, leading to longer response times or missed alarms2.
* Alarm fatigue can compromise patient safety by increasing the risk of adverse events, such as delayed treatment, missed diagnosis, or cardiac arrest3.
* To reduce alarm fatigue, the Joint Commission recommends a four-step approach: establish alarm system management as a priority; identify the most important alarms to manage; establish policies and procedures for alarm system management; and educate staff and patients about alarm system management4.
* The most appropriate first intervention for an event related to a delayed high-priority alarm response is to review alarm signals for clinical appropriateness. This means to evaluate the alarm settings, limits, and delays for each device and patient population, and adjust them according to evidence-based guidelines and best practices5. This can help reduce the number of false or clinically insignificant alarms, and improve the specificity and sensitivity of the alarm system.
* Establishing a written policy for alarm escalation is also an important intervention, but it is not the first step. A policy for alarm escalation should define the roles and responsibilities of staff, the criteria and process for escalating alarms, and the expected response time and actions for each alarm level.
However, before developing such a policy, it is necessary to review the alarm signals and ensure that they are clinically relevant and meaningful.
* Implementing a guideline with clear criteria for initiation of cardiac monitoring is another intervention that can reduce alarm fatigue, but it is not the first step either. A guideline for cardiac monitoring should specify the indications, duration, and discontinuation of continuous electrocardiographic (ECG) monitoring for patients at risk of cardiac arrhythmias or ischemia. However, before implementing such a guideline, it is necessary to review the alarm signals and ensure that they are appropriate for the patient population and clinical setting. References: 1: NAHQ Code of Ethics 2: Reducing the Safety Hazards of Monitor Alert and Alarm Fatigue 3: Alarm fatigue: impacts on patient safety 4: The Joint Commission National Patient Safety Goal on clinical alarm safety 5: Alarm Management: Advancing From Failure Cause To Root Cause Analysis : [Utilization of Improvement Methodologies by Healthcare Quality Professionals During the COVID-19 Pandemic] : [The Financial Case for Quality as a Business Strategy] : [Shaping the Future of the Healthcare Quality Profession] : [Practice Standards for ElectrocardiographicMonitoring in Hospital Settings] : [Understanding the Evolving Landscape of Healthcare Quality]
NEW QUESTION # 177
A department director has been asked to compare the productivity of the department with the productivity of similar departments at other facilities.
Which of the following Is the first step of this project?
- A. Determine which processes will be evaluated,
- B. Review department Job descriptions with another facility of similar size.
- C. Conduct a search on the Internet for guidelines.
- D. Monitor the work flow in the department for at least six months.
Answer: A
Explanation:
When comparing the productivity of a department with similar departments at other facilities, the first step is to determine which processes will be evaluated1. This involves identifying the key processes that contribute to the department's productivity and are comparable across different facilities1. Once these processes are identified, they can be measured and compared to similar processes at other facilities1.
This comparison can provide valuable insights into areas where the department is performing well and where there may be opportunities for improvement1.
Reference: https://www.indeed.com/career-advice/career-development/benchmarking-in-health-care
NEW QUESTION # 178
Which of the following should a healthcare plan use to collect satisfaction data from its health plan members?
- A. disease data obtained from disease registries
- B. data collected through questionnaires or surveys
- C. claims data obtained from healthcare payors
- D. data collected from the electronic health record
Answer: B
Explanation:
To collect satisfaction data from its health plan members, a healthcare plan should use data collected through questionnaires or surveys. Surveys are a direct method of gathering feedback from members about their experiences, perceptions, and satisfaction with the health plan. This data is essential for understanding the strengths and weaknesses of the plan from the members' perspective, which can then be used to make improvements.
Claims data obtained from healthcare payors (B): Claims data provides information on services used but does not directly measure member satisfaction.
Disease data obtained from disease registries (C): Disease data tracks health outcomes but is not related to satisfaction.
Data collected from the electronic health record (D): EHR data includes clinical information but does not capture member satisfaction directly.
Reference
NAHQ Body of Knowledge: Patient and Member Satisfaction Measurement
NAHQ CPHQ Exam Preparation Materials: Collecting and Analyzing Satisfaction Data
NEW QUESTION # 179
Because of their detail and straightforward design, patient registries are a powerful source of quality improvement data. Registries usually are specialty or procedure specific.
For instance (Choose two):
- A. Total joint replacement
- B. Patient's bile test
- C. Enrollment in disease management program
- D. Acute myocardial infraction
Answer: A,D
NEW QUESTION # 180
A quality improvement coordinator is asked to develop a training session on team facilitation based on adult learning principles. Which of the following would be the best approach to include?
- A. Ask participants to study facilitation techniques after class.
- B. Ask participants to practice facilitation with the group during class.
- C. Teach all the concepts and test participants at the end of class.
- D. Teach the basic concepts and handout printed slides for participants to refer to after class.
Answer: B
Explanation:
When developing a training session based on adult learning principles, it is crucial to engage learners actively and make the learning experience as practical and relevant as possible. Here's why option A is the best approach:
* Active Participation:
* Adult learners benefit most from hands-on learning where they can apply concepts immediately.
Practicing facilitation during the class allows participants to actively engage with the material, which enhances learning retention.
* Immediate Application:
* Adult learning theory emphasizes the importance of immediate application of skills. By facilitating within the group during class, participants can receive instant feedback, allowing them to refine their skills in real-time.
* Experiential Learning:
* This approach aligns with Kolb's experiential learning cycle, which involves concrete experience, reflective observation, abstract conceptualization, and active experimentation.
Facilitating in class provides the concrete experience and opportunity for reflective observation.
* Peer Learning and Feedback:
* Practicing in a group setting allows for peer learning, where participants can observe others and learn from their approaches. Feedback from peers and the facilitator is also crucial in developing effective facilitation skills.
Other options (B, C, and D) are more passive approaches, which are less effective in adult learning as they do not engage participants in the active, experiential learning process that is critical for skill development.
References:
* NAHQ's Principles of Adult Learning in Healthcare Education
* NAHQ Guide to Effective Training and Education in Healthcare
=========
NEW QUESTION # 181
Which of the following are the most important characteristics of quality metrics?
- A. Statistical, random, and feasible
- B. Valid, reliable, and feasible
- C. Random, unbiased, and reactive
- D. Repeatable, reliable, and reactive
Answer: B
Explanation:
Quality metrics must be valid, reliable, and feasible to be useful and meaningful in healthcare performance improvement. Validity ensures the metric measures what it intends to measure, reflecting true aspects of quality care. Reliability means the metric produces consistent results across different observers and over time, essential for credible comparisons and trend analysis. Feasibility means data can be collected with reasonable effort and cost, enabling regular monitoring and timely decision-making (The Joint Commission, Measurement Standards, 2024; National Quality Forum, Measure Evaluation Criteria, 2024). Without these qualities, data can mislead or fail to drive improvement. For example, a metric lacking validity may not reflect actual patient outcomes, while unreliable data can produce conflicting results, undermining trust. Feasibility is critical to ensure sustainable quality measurement systems. Other options like "random" and "reactive" are less relevant: metrics should be systematic and proactive rather than reactive. This triad of characteristics is emphasized in accreditation standards and quality improvement frameworks.
References:
The Joint Commission, Measurement Standards, 2024
National Quality Forum (NQF), Measure Evaluation Criteria, 2024
NEW QUESTION # 182
Which of the following will help determine the health status of a defined population?
- A. Rate of preventive health care visits found by reviewing claims data
- B. Demographics such as age, race/ethnicity, and socioeconomic status
- C. Frequency of chronic disease as reported by patients in a clinic
- D. Percentage of individuals with a higher education degree
Answer: B
Explanation:
Demographic factors like age, race/ethnicity, and socioeconomic status are fundamental in assessing the health status of a population. The NAHQ CPHQ Detailed Content Outline underlines the necessity of analyzing such data to identify health disparities and target improvement efforts effectively.cdn.nahq.org Understanding these demographics enables healthcare professionals to tailor interventions and allocate resources to areas where they are most needed, thereby enhancing population health outcomes.
NEW QUESTION # 183
An ambulatory care practice has reviewed data to identify patients with multiple visits to the emergency room within the last six months. The population health management technique for this type of data review is called
- A. Hot-spotting
- B. Syndromic surveillance
- C. Public health surveillance
- D. Cold-spotting
Answer: A
Explanation:
Population health management uses data to identify and target high-risk or high-utilization patients for interventions to improve outcomes and reduce costs.
Option A (Cold-spotting): Cold-spotting identifies areas or populations with low healthcare utilization, not relevant to high ER use.
Option B (Hot-spotting): This is the correct answer. The NAHQ CPHQ study guide states, "Hot-spotting is a population health technique that identifies patients with high healthcare utilization, such as frequent ER visits, for targeted interventions" (Domain 5). Developed by Dr. Jeffrey Brenner, it focuses on high-cost, high-need patients.
Option C (Syndromic surveillance): This monitors disease patterns (e.g., flu outbreaks), not individual utilization.
Option D (Public health surveillance): This tracks population-level health trends, not individual high utilizers.
CPHQ Objective Reference: Domain 5: Population Health and Care Transitions, Objective 5.2, "Apply population health management techniques," includes hot-spotting for high-risk patients. The NAHQ study guide notes, "Hot-spotting targets high-utilization patients to reduce costs and improve care" (Domain 5).
Rationale: Hot-spotting directly addresses frequent ER users, aligning with CPHQ's population health strategies.
Reference: NAHQ CPHQ Study Guide, Domain 5: Population Health and Care Transitions, Objective 5.2.
NEW QUESTION # 184
Feedback from patients and their families will provide rich information for quality improvement work.
For these efforts to be successful, you should consider the some questions.
Which of the following is NOT out of those questions?
- A. What is your aim for improvement?
- B. Who will review the data?
- C. What was your last year budget?
- D. How frequently do you need to measure your performance to achieve your name?
Answer: C
NEW QUESTION # 185
What is the best method to communicate detailed patient experience scores?
- A. Discuss the information at unit level meetings.
- B. Disseminate the information in a publication.
- C. Disseminate organization-wide via email.
- D. Present the information at general meetings.
Answer: A
Explanation:
Detailed Explanation:
Discussing patient experience scores at unit-level meetings is the most effective way to ensure that detailed feedback reaches staff directly involved in patient care. Unit-level discussions allow for targeted discussions, specific action planning, and immediate feedback.
Option C: Discuss the information at unit level meetings
Unit meetings are ideal for addressing specifics relevant to each team, enabling them to understand and act on the data.
Other Options:
General meetings and organization-wide emails provide less specificity and may not reach or engage frontline staff effectively.
References:
Quality improvement literature emphasizes the importance of engaging frontline staff in unit-level feedback to directly influence patient experience.
NEW QUESTION # 186
......
New 2026 Realistic Free NAHQ CPHQ Exam Dump Questions and Answer: https://www.fast2test.com/CPHQ-premium-file.html
NAHQ CPHQ Exam: Basic Questions With Answers: https://drive.google.com/open?id=1xUcYskfMV-vskfdrubGBNYBrlCwr_fMt